

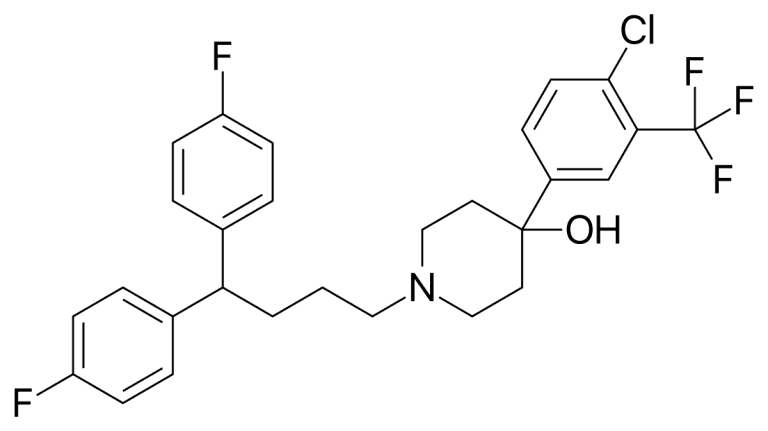
Penfluridol is a very potent first-generation diphenylbutylpiperidine antipsychotic drug discovered by researchers at Janssen Pharmaceutica in 1968.
Psychiatrists and related medical practitioners prescribe penfluridol for antipsychotic treatment of chronic schizophrenia and related psychotic disorders. While many practitioners are replacing it with atypical “second-generation” antipsychotics, it remains in use as a low-cost intervention for the treatment of schizophrenia and other psychotic disorders diagnosed by psychiatrists.
Other names and related medications
Other names for penfluridol include Semap, Micefal, & Longoperidol. Other diphenylbutylpiperidine antipsychotics related to penfluridol include pimozide and fluspirilene.
Conditions Treated
Penfluridol is prescribed to treat schizophrenia. Researchers have also identified the drug as a possible anticancer agent.
Schizophrenia treatment with penfluridol
Schizophrenia is a mental disorder diagnosed by psychiatrists that is characterized by the inability to interpret reality “normally”. Along with what is classified as “extremely disordered thinking and behavior”, schizophrenia is believed to produce a combination of delusions and hallucinations that may impair daily activities and even result in disability.
Mental health professionals and researchers generally do not know what causes schizophrenia. According to the industry, typical factors include genetics, brain chemistry and environmental conditions.
Researchers generally believe that imbalances in some naturally occurring brain chemicals such as dopamine and glutamate contribute to the condition. Accordingly, neuroimaging studies have shown differences in the central nervous system and brain structure of people diagnosed with schizophrenia. While the nature of those differences is not clear, researchers believe that variances in the central nervous systems and brain structure of people diagnosed with schizophrenia indicate that it is a brain disease. Some mental health professionals believe that schizophrenia requires lifelong treatment. They also believe that serious complications can be reduced if the condition is identified early.
Medications are the “cornerstone” of schizophrenia treatment, according to the Mayo Clinic, and are used to manage signs and symptoms using the lowest dose possible. Prescribed by psychiatrists, these drugs are prescribed in different doses and combinations over time to achieve the desired results. They are also combined with anti-anxiety medications in some cases.
Penfluridol as an anti-cancer agent
A study on penfluridol explored its possible use as a novel anti-cancer agent. This was demonstrated through its ability to inhibit the growth of Panc-1, BxPC-3 and AsPC-1 pancreatic cancer cells in a concentration-dependent manner, leading to apoptosis, induced ER stress and autophagy. Accordingly, penfluridol was researched in a separate study that suggested it can inhibit tumor growth in vivo as well as act cytotoxic to cancer cells in vitro. Researchers postulated that the drug’s anti-cancer properties might be attributed to a dysregulation of cholesterol homeostasis, leading to its involvement in anti-tumor mechanisms.
How it Works
Penfluridol is a neuroleptic drug that is reported to relieve positive and negative schizophrenia symptoms.
It works by inhibiting the binding of dopamine to dopamine receptors with Ki of 1.6 μM, and exerts antipsychotic activity by blocking limbic system and mesocortical area dopamine projections. It has also been shown to selectively inhibit the [3H]nitrendipine binding to rat cerebral cortical membrane fraction while competitively antagonizing potassium-induced calcium-dependent contractions in rat vas deferens. It additionally inhibits the contractile response of isolated rings of rabbit thoracic aorta to NE and KCl while inhibiting calcium influx during either KCI or NE stimulation.Get your requested
raw materials
quotation
Treatment Outcomes
An analysis of penfluridol studies determined that there is enough consistency to establish different outcomes. The report determined that the adverse effects and overall effectiveness of penfluridol are similar to other common antipsychotic medications.
The studies demonstrated that Penfluridol was a satisfactory way to treat the symptoms of schizophrenia, particularly for those that did not adapt adequately to depot drugs or respond well to daily oral medication. When compared to depot antipsychotic medications, penfluridol was shown to have a lower drop-out rate in the medium term. The studies also suggested that Penfluridol was a suitable option for individuals suffering from long-term schizophrenia with residual psychotic symptoms that required antipsychotic medication on a continued basis.
Research Studies
A recent analysis of research studies on penfluridol examined 25 studies that totaled 1024 participants, undertaken in the 1970s following the launch of penfluridol.
A total of ten studies with 365 patients compared a placebo to penfluridol. Penfluridol was superior to placebo in a meta‐analysis of medium‐term lasting studies in the following main efficacy measures: ‘improvement in global state’ (n=159, 4 RCTs, RR 0.69 CI 0.6 to 0.8, NNT 3 CI 2 to 10) and ‘needing additional antipsychotic’ (n=138, 5 RCTs, RR 0.43 CI 0.2 to 0.8, NNT 3 CI 1.8 to 20).
Eleven studies totaling 449 patients randomized penfluridol and oral typical antipsychotics. The results showed that there were not any particular differences between penfluridol and either fluphenazine, chlorpromazine, trifluoperazine, thiothixene or thioridazine in the medium term for the following main outcome measures: ‘improvement on global state’ (N=2 studies), ‘leaving the study early’ (N=6), ‘needing additional antipsychotic’ (N=3), needing antiparkinsonian medication (N=2), and side‐effects.
Finally, six studies of 274 patients compared depot typical antipsychotics to penfluridol. While no differences were established for efficacy and safety measures, penfluridol was shown to be superior for maintaining patients in treatment: ‘leaving the study early’ (n=218, 5RCTs, RR 0.55 CI 0.3 to 0.97, NNT 6 CI 3.4 to 50).
Typical Dosage
Penfluridol’s effects last for many days after a single oral dose due to its very long elimination half-life with similar effects to pimozide and haloperidol. It is typically prescribed as an oral weekly dose of 10–60 mg as a result of its very long-lasting effect.
A notable study compared a weekly penfluridol dose with a daily chlorpromazine dose in 56 outpatient schizophrenic patients. The results determined that the doses of both drugs were similar in their clinical effectiveness with no major difference in side effects.
Side Effects
Side effects of penfluridol include sedation, akathisia, dyskinesia, “pseudo”-Parkinsonism, abnormal voluntary movements, constipation, increased prolactin blood level, mouth dryness, muscle stiffness, sleepiness, tremors, orthostatic hypotension (sudden blood pressure lowering after standing), weight gain and urinary retention.
Contraindications
The use of penfluridol is contraindicated in patients that have pre existing central nervous system depression or coma.Get your requested
raw materials
quotation

